The Patient/Advocate Oncology Passport
Patient Advocate AI Use Case
The Patient/Advocate Oncology Passport
Could AI Help Patients Arrive Better Prepared for Clinical Trials?
This is not medical advice.
This is not a proposal to let AI decide whether a patient qualifies for a clinical trial or replace doctors, coordinators, nurses, principal investigators, pathologists, pharmacists, or trial teams.
The idea is simpler:
Could AI help create a better first draft?
Could it organize the records a patient already carries?
Could it help patients and trial teams begin from a clearer starting point?
Patients Arrive Carrying Too Much
Cancer patients rarely arrive at a clinical trial with one clean story.
We arrive with a range of documents: pathology reports, scans, lab results, medication lists, treatment histories, molecular testing, ctDNA results, side effects, and unanswered questions.
Some information lives in portals, PDFs, clinical notes, pathology departments, or imaging systems. Some lives only in the patient’s memory, which may be strained by surgery, treatment, fatigue, fear, and sleepless nights.
By the time a patient reaches a trial conversation, we may have enough records to qualify as a small, poorly organized medical library.
Patients are often asked to become information fusers. In practice, it can feel like trying to assemble an airplane from a range of medical documents while it is already in the air.
That is difficult on a good day.
It is harder when you are sick.
From Molecular Passport to Patient/Advocate Oncology Passport
A Molecular Passport summarizes the tumor’s biology: genomic findings, biomarkers, target expression, ctDNA, tissue availability, and assay results.
That is useful, but the idea should be wider.
The Molecular Passport describes the tumor.
The Patient/Advocate Oncology Passport describes the person carrying it.
A patient entering a trial is more than a tumor profile. The trial team may also need to understand treatment history, current condition, prior toxicities, safety concerns, communication needs, support systems, open questions, and practical barriers.
The science matters.
The person matters too.
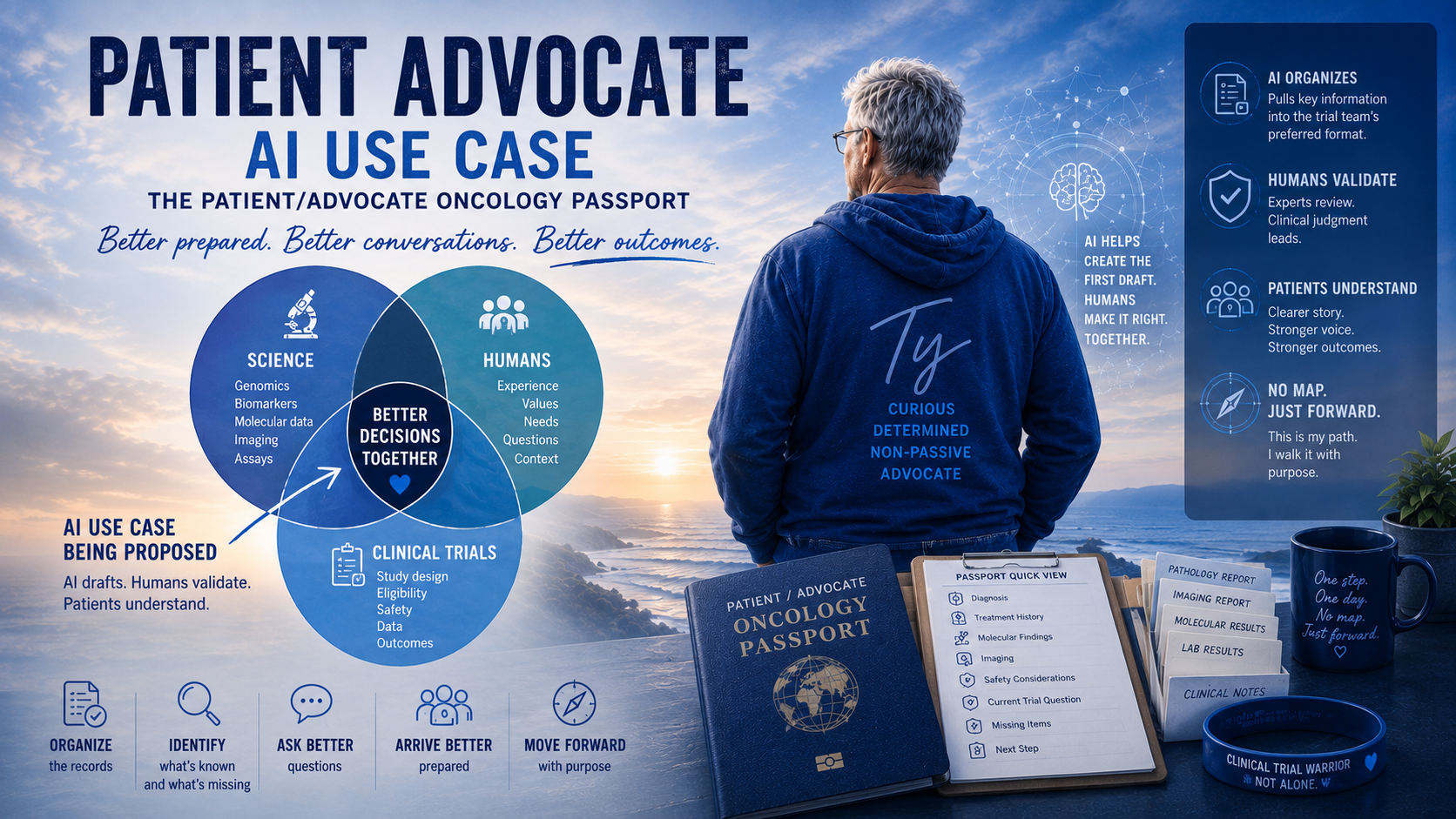
The AI Use Case
The trial team should provide the Passport format first.
Not a generic form. Not whatever the patient or AI invents.
The actual structure the team would find useful.
It might include:
required fields and preferred terminology;
molecular and eligibility-related categories;
prior-treatment history;
source-document requirements;
rules for missing, conflicting, or unconfirmed information;
support and communication needs;
trial-specific screening questions.
AI could then draft a Patient/Advocate Oncology Passport from the patient’s existing records.
The draft would not be final or treated as medical truth. It would go to the patient and appropriate members of the care or trial team for review and validation.
In plain English:
AI drafts.
Humans validate.
Patients understand.
That is the guardrail.
What AI Should Not Do
AI should not:
decide final eligibility;
replace clinical judgment;
recommend treatment;
invent missing information;
hide uncertainty;
make conflicting records appear consistent;
turn hope into a false conclusion.
Clinical judgment must remain with qualified people.
What AI Might Help Do
AI may be useful as an organizer, sorter, translator, and draft builder.
It might help:
create a treatment timeline;
summarize prior therapies;
identify recent imaging and pathology;
extract molecular and ctDNA results;
separate verified records from patient-reported information;
flag missing or conflicting information;
build a plain-language glossary;
draft questions for the study team;
create a “who has the ball?” status list;
place information into the team’s preferred format.
That could reduce the blank-page problem and help everyone begin with a clearer draft.
A Possible Passport Structure
The Passport might have two layers.
Layer One: One-Page Quick View
A page a busy clinician or coordinator can scan quickly:
patient and treating-oncologist information;
diagnosis and current disease status;
major treatment history;
most recent imaging;
known molecular findings;
major safety concerns;
current trial question;
missing items;
next step.
Not the whole story.
Just enough to prevent the first conversation from starting blind.
Layer Two: Supporting Details
This could include:
full treatment timeline;
surgeries and radiation;
prior systemic therapies;
side effects, reactions, and treatment limitations;
pathology and imaging summaries;
genomic and ctDNA results;
biomarkers;
tissue-block location;
medications and allergies;
caregiver and support information;
communication and learning preferences;
practical barriers;
questions for the trial team.
The goal is practical clarity, not medical perfection.
Verified, Patient-Reported, or Missing
Each important item should be labeled clearly:
Verified from a source document
The information comes from an official report, assay, scan, or clinical note.
Patient-reported
The patient supplied it, but the team may still need to confirm it.
Missing or needs confirmation
The information matters but is not yet available or validated.
This protects the science while allowing patients to contribute useful information.
It also prevents AI-generated language from sounding more certain than the records justify.
The Trial Team’s Format Comes First
If every patient creates a different Passport, the study team may receive ten different versions of confusion.
The team should define the structure first. AI should organize the patient’s information into that structure.
That makes the Passport a bridge, not another burden.
A Passport would not replace expert judgment. Like a good checklist, it would help expert judgment begin with the right information in view.
Fitting Within Existing Trial Infrastructure
Centers such as UC San Diego Moores Cancer Center already have serious clinical-trial infrastructure, including research support, study-design resources, monitoring, patient-care follow-up, and translational research services.
The Passport would not replace that work.
It would serve as a patient-side companion: a cleaner first draft in the team’s preferred format, ready for human review.
No one is asking AI to drive the bus.
At most, it helps gather the luggage, label the bags, and makes sure the map is not upside down.
Why This Might Help Patients
The Passport could help patients:
understand their own story;
see what is known and what is missing;
ask better questions;
arrive less scattered and better prepared.
That may not mean less afraid.
But perhaps less lost.
Sometimes less lost is a very big thing.
The Passport is not meant to make the patient sound like a doctor. It is meant to keep the patient from arriving like a mystery wrapped in a records request.
Why This Might Help Trial Teams
For study teams, the Passport could:
reduce repeated information gathering;
make preliminary review cleaner;
identify missing records sooner;
show what information is already available;
bring patient needs into the process more clearly.
Trial participation is not only about whether a tumor matches a protocol.
It is also about whether the person can safely, realistically, and knowingly walk the trial road.
My Own Lens
I am not proposing this as an AI expert or medical researcher.
I am proposing it as a cancer patient who has had to learn too many terms too quickly.
I also bring experience as a former principal investigator on a federally funded research-and-development program, a degree in Human Communications, and personal experience with dyslexia.
That does not make me an expert in clinical-trial operations.
But it does make me sensitive to one problem:
The right information can exist and still not be usable when someone needs it.
That is a design problem.
The Passport is one possible response.
A Human-Centered Workflow
Step 1: The trial team defines the template
The team decides what information is useful for screening, communication, education, and trial entry.
Step 2: The patient supplies or authorizes access to records
These may include pathology, imaging, molecular assays, treatment history, medications, and patient notes.
Step 3: AI creates a draft
The information is organized into the team’s format and labeled as verified, patient-reported, missing, conflicting, or awaiting confirmation.
Step 4: The patient reviews it
The patient corrects obvious errors and adds questions, support needs, and practical concerns.
Step 5: The study team validates it
Appropriate trial personnel confirm what is usable and what still needs correction or documentation.
Step 6: The Passport becomes a living document
It can be updated after scans, biopsies, assays, eligibility decisions, or changes in the patient’s condition.
The goal is not automated eligibility.
The goal is better-prepared human review.
Questions Worth Asking Before Building It
Before developing this AI use case, I would ask:
What information do coordinators need first?
What slows preliminary review?
Which records are most useful early in the process?
Which fields require formal validation?
How should missing or conflicting information appear?
Could the Passport reduce duplicate record requests?
Could it help patients understand who has the ball?
How could it work better for dyslexic, fatigued, chemo-brained, or overwhelmed patients?
How could it remain useful without creating more work for trial teams?
Those are design questions.
Good trials deserve good design questions.
AI Experiment
I designed a simple AI prompt to review all of my medical data and format a table of my imaging for the past two years. The table is searchable, and can be sorted by who ordered the imaging, what type they ordered (PET CT, CT, etc), Contrast (Y/N) and other data. What I found was fascinating. surgeon was watching my cancer with PET scans, until he turned my care over to an Oncologist who used CT scans. What was caught? What was Missed. Is this following protocols? I did find the tabular format very useful for asking questions, and for some overview and discovery of my care.
Closing Thought
The Patient/Advocate Oncology Passport would not replace the medical record, doctor, coordinator, principal investigator, trial team, or patient.
Its purpose would be practical:
Help organize the patient’s story in the team’s preferred format.
Show what is known, missing, or unconfirmed.
Help the patient arrive better prepared.
Help the study team begin with a cleaner draft.
Help everyone spend less time hunting for the map and more time deciding what it means.
Precision medicine should not stop at the tumor.
It should include the patient.
With the right guardrails, this patient-advocate AI use case may help build the first draft of that bridge.
—Ty
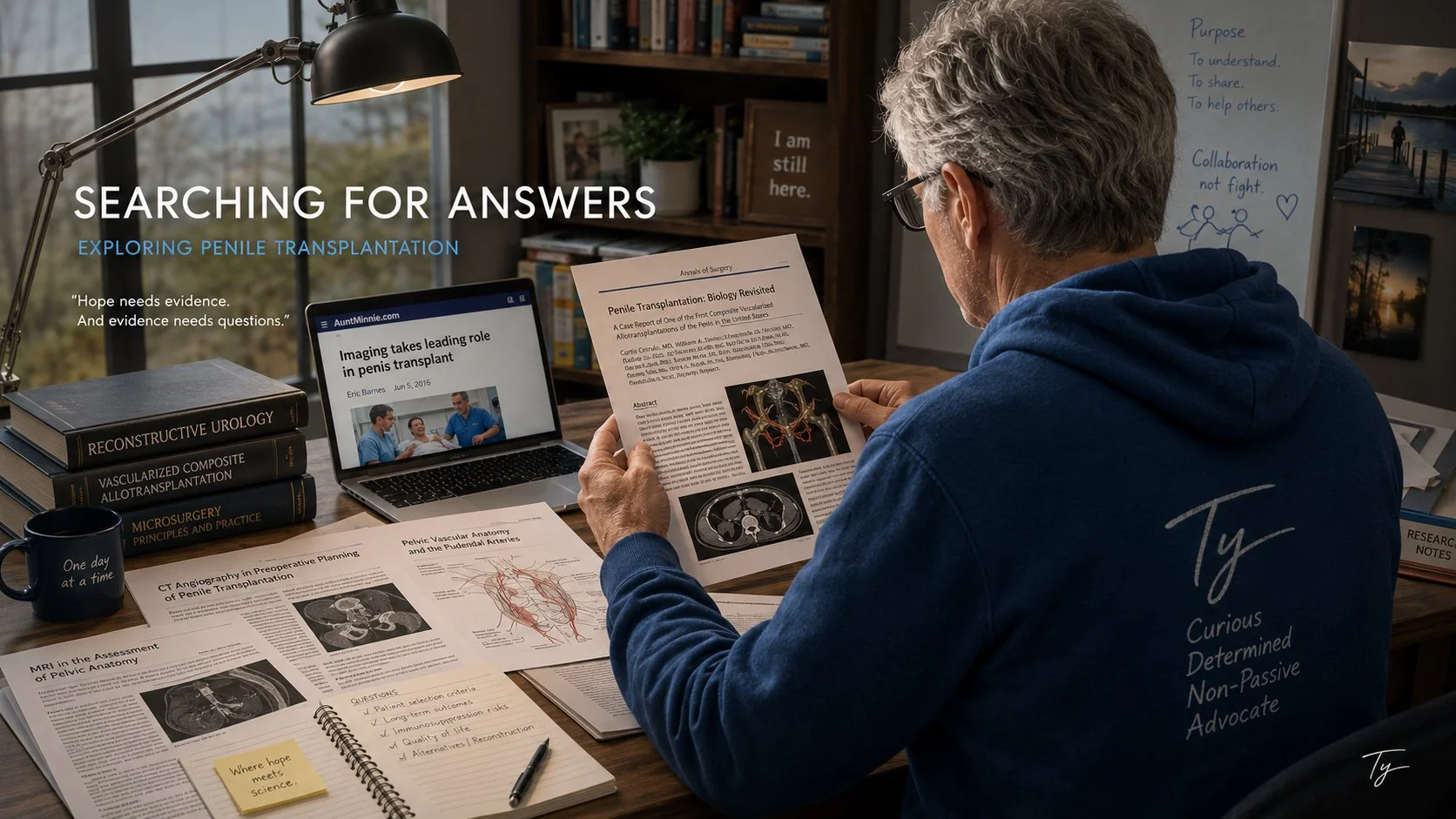
Is Penis Transplantation A Thing?
“Penis Transplantation After Penile Cancer:
Real Medicine, Experimental Frontier, or Both?”
In 2016, an article by medical-imaging journalist Eric Barnes described one of the most unusual reconstructive operations ever attempted: the first penis transplant performed in the United States. The recipient, Thomas Manning, had undergone a partial penectomy after penile cancer. Surgeons at Massachusetts General Hospital attached a penis from a deceased donor during a complex operation involving blood vessels, nerves, erectile tissue, the urethra and skin.
The article, “Imaging Takes Leading Role in Penis Transplant,” focused especially on the use of CT angiography, conventional angiography and MRI to help the surgical team study the recipient’s anatomy and plan the procedure. The account was published by AuntMinnie.com on June 5, 2016, shortly after the operation.
At first glance, the procedure can sound almost too extraordinary to be credible. But the basic event was real, and it was not simply a sensational news story. Massachusetts General Hospital.
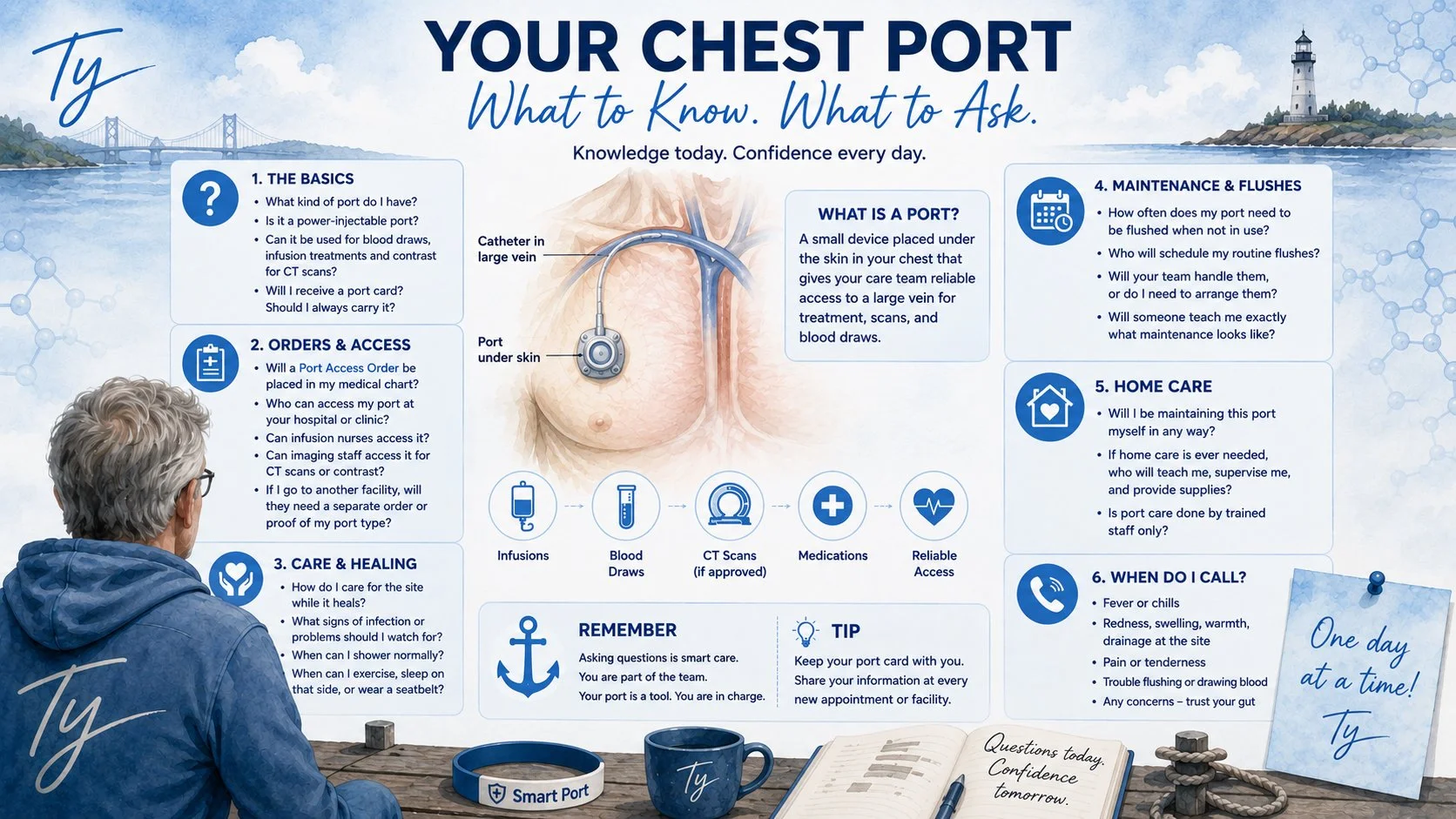
Learning: My New Port
Getting a port placed in my chest was not just a procedure. It was the beginning of learning an entirely new piece of medical equipment that will become part of my everyday cancer care. A port may sit quietly beneath my skin in my chest, but it carries important details: its manufacturer, model, construction material, catheter type, pressure limits (mine is rated for 300PSI), flow rate, imaging compatibility, and maintenance requirements. I have learned that knowing those details is not unnecessary medical trivia. It helps me ask better questions at infusion centers, imaging departments, emergency rooms, and every new facility where someone may need to access my port.
Before I go further, I want to be clear that I have no financial, professional, or promotional relationship with AngioDynamics, maker of my port. I am using the company and its products as an example because AngioDynamics manufactured the port that was implanted in me. Other manufacturers make implantable ports, and patients should always follow the instructions for their own specific device and care team.
For additional product specifications, model information, UPN listings, pressure and flow-rate details, and SmartPort CT identification features on my device, you can review the company’s product brochure:
View the AngioDynamics SmartPort brochure
My port is an AngioDynamics SmartPort CT Low-Profile titanium port. In the AngioDynamics product catalog, low-profile titanium models have UPNs (Unique Product Numbers) containing “LT”. I looked it up online and found out my port body is made from medical-grade titanium, while the catheter material may differ according to the exact model. The complete UPN on the implant record, product sticker, or patient identification card is therefore more useful than simply saying, “I have a SmartPort.”
The Patient Port Packet I Procured.
After my port was placed, I was given a small patient packet. At first glance, it looked like the kind of paperwork that could easily be set aside and forgotten. I quickly realized that it contained some of the most important information about the medical device now sitting beneath my skin.
The packet included:
A patient checklist
A blue-and-white silicone wrist bracelet identifying a Power Injectable Port and Smart Port
A sticker containing the port’s complete UPN code
A wallet-sized patient identification card
A smaller snap-off key-ring identification card
The model and identifying details of my port
A UCSD point of contact and telephone number for product or clinical questions
That wallet card should not live forgotten in a drawer. It should be carried and shown to anyone who plans to access the port. It gives the clinician important information about the model, pressure rating, flow limitations, and manufacturer. The smaller key-ring card provides an additional way to keep identification information nearby.
My practical approach is redundancy. I keep the physical card, photograph both sides of it, save the information on my phone, and make sure the details are included in my medical record. Phones lose power, patient portals can be incomplete, and different medical systems do not always communicate with one another.
The Port Patient App
AngioDynamics also offers a Port Patient App for people with its implantable ports. The app is available through the Apple App Store for iOS devices and Google Play for Android devices. It can be found by searching for “AngioDynamics” from a mobile device.
The app serves as a portable repository for information that may be needed during medical visits, including:
The model of the implanted port
The port’s maximum pressure and flow-rate specifications
Product-support information
The implantation date
Dates of previous procedures
The person that placed the port for me.
That information can be valuable when arriving at a new infusion center or imaging clinic where staff may not immediately see the full implant record.
I would still carry the physical identification card even when using the app. The best system is the one with backups: the app, the wallet card, a photograph of the card, and documentation in the chart.
What Makes the SmartPort CT Different?
From their website, the SmartPort CT family is designed for repeated vascular access, including medications, fluids, blood products, blood sampling, and—in approved circumstances—the power injection of contrast for imaging.
My specific port is rated for power injection at up to 300 PSI for contrast and other approved fluids used during my CT scans. That does not mean anyone should simply connect to it and begin an injection. The exact model must first be confirmed, the proper needle and technique must be used, and the imaging facility. Lab or infusion center must follow its own policy and the manufacturer’s instructions.
A power-injectable port is useful because it may reduce the need for a separate peripheral IV during a CT scan. But “power-injectable” is only part of the answer. The care team still needs to verify the device, confirm that the port is functioning properly, and ensure that the staff member accessing it is trained and authorized to do so.
Smart Angle Identification: The Port Can Be Recognized on Imaging
One feature I found especially interesting is the way SmartPort power-injectable ports can be identified on medical imaging.
SmartPort power-injectable ports can be identified by Smart Angle technology on the CT, CT Low-Profile, and Plastic CT models. The CT engraving on all models can be identified through a chest X-ray or CT scout scan.
Amazing.
That means the port does not rely only on a paper card or a patient remembering the model name. Its identifying features may also be visible on imaging. This can give clinicians another way to recognize that the device is a power-injectable SmartPort.
Even with that imaging feature, I would still want the complete model, UPN, pressure rating, and implant information confirmed before the port is used for power injection. Imaging identification is helpful, but it should work alongside the patient card, medical chart, manufacturer information, and facility safety procedures.
Vortex Technology: A Different Kind of Chamber
One of the features that interested me most was Vortex Technology. Rather than using a chamber with a perpendicular outlet, the Vortex design has a round reservoir and a tangential, or offset, outlet. Fluid enters in a way that creates a circular flushing action through the chamber.
The goal is to allow fluid to reach more of the chamber’s internal surface, reduce stagnant spaces, resist sludge buildup, and lower the possibility of an occlusion. The round chamber and offset outlet are designed to create a more complete flushing action inside the reservoir.
AngioDynamics cites a clinical study in which Vortex chamber ports were associated with a 73% reduction in port occlusions and 69% fewer secondary interventions compared with conventional ports. The company also cites an estimated average saving of $1,224 per patient compared with conventional ports. These are manufacturer-presented findings and should not be interpreted as a guarantee of what any individual patient will experience.
The newer AngioDynamics SmartPort+ platform combines Vortex chamber technology with additional catheter technology intended to resist thrombus accumulation. Vortex remains one of the key design features that distinguishes the port chamber itself.
A Port Can Be “Power-Injectable” and Still Require Questions
When I hear that my port is power-injectable, my next question is not simply, “Can you use it?” The questions I asked myself:
Has the exact model and UPN been confirmed?
Have I reviewed my port identification card?
At the Lab, I will ask if the port is currently functioning properly and giving blood return?
For the person accessing my port: are you using the manufacturer-approved power-injection needle and technique? A non-boring needle needs to be used.
Is there a Port Access Order in my medical chart?
Is the nurse or imaging clinician credentialed under the facility’s policy to access it?
What maximum flow rate and pressure apply to my exact port?
Will this facility use my port for CT contrast, or will it require a separate peripheral IV? I have a fried with a port and a PICC line, so asking if that is a possibility may be import to learn.
A device may be capable of something while a particular clinic is not authorized or equipped to perform it. Device approval, clinical orders, staff training, and facility policy all have to meet in the “same room.”
The card included in my patient packet will be shown to anyone who is going to access my port. It contains the details needed to confirm what the device is and how it may safely be used. It also provides a contact name and department (Interventional Radiology, IR) and a telephone number in case the clinician needs additional information.
Learning the CPT Codes
Here’s a related bit of information… Another part of the process that I found surprisingly valuable was learning about Current Procedural Terminology, or CPT, codes. CPT codes are used to describe medical procedures and services, and they can affect prior authorization, billing, and how an insurer evaluates a claim.
I learned to double-check which codes had been requested and approved for each procedure. That helped me form better questions before arriving:
Which CPT codes are being submitted for this procedure?
Were all necessary primary and add-on services included in the authorization request?
Does the approval cover the facility, physician, imaging guidance, anesthesia, and other separately reportable services?
Does the insurer’s authorization guarantee coverage, or could coding and medical-necessity rules still affect payment?
An authorization is important, but it is not always a promise that every component will be paid. Coding rules can also vary depending on the procedure, payer, documentation, and whether a service is considered bundled into another code. In my partial penectomy, by reviewing the codes I found my surgeon’s promise of at least one night in the hospital was not backed up by the billing (CPT) codes. After phone calls, I finally rescheduled surgery for the following week, with the proper codes included in the orders. CPT codes as far as I know are for the US, and I am not sure what type of billing or authorization codes are used in other locations.
CPT Code 76937: An Example of an Add-On Service
A useful example is CPT code 76937, which represents ultrasound guidance for vascular access procedures, such as central-line or arterial-line placement, meaning a port placement in my case.
It is an add-on code, meaning it must be reported in addition to the primary procedure rather than billed as a stand-alone service. It also requires specific documentation, including:
Confirmation that the selected vessel is open
Concurrent, real-time ultrasound visualization of the needle entering the vessel
Permanent image recording
An appropriate written report
Some procedures already include imaging guidance, and payer rules may prevent separate payment in certain circumstances. That is why the code should be confirmed by the clinical coding team and insurer rather than assumed to apply automatically. I found I could call my insurance company and they helped me understand my codes.
This is exactly why learning a little about CPT codes helped me. I was not trying to become a medical coder. I was trying to make sure that the procedure my physician ordered, the services the team expected to perform, and the services the insurer authorized were all describing the same event.
The Information I Want in My Own Record
For my own SmartPort, I want my medical chart and my personal records to include:
Manufacturer: AngioDynamics
Product family: SmartPort CT
Configuration: low-profile, single lumen
Port-body material: medical-grade titanium
Complete UPN and catheter details
Implantation date and implanting facility
Power-injection rating of 300 PSI
Maximum approved flow rate
MRI-conditional information
Port Access Order, when required
Maintenance and flushing schedule
Who may access it at infusion and imaging facilities
Product-support contact name and telephone number
I also look forward to my doctor providing a Port Maintenace procedure and schedule.
The port itself may be small, but the information surrounding it is not. Knowing the model, understanding what “power-injectable” really means, keeping the patient packet, installing the phone app, wearing the wristband when I am away from home, carrying the D card, and having the UPN information available, and asking about CPT codes all give me a clearer role in my own care.
Cancer already comes with enough uncertainty. I cannot control every part of it. But I can learn the name of the device in my chest, understand how it was designed, carry the information that explains it, and make sure the right questions are asked before someone accesses it.
One day at a time. One question at a time.
—Ty
Molecular Tumor Boards: Where the Room Gets Bigger
This blog entry came from research into the evolution from Tumor Boars to Molecular Tumor Boards. UCSD in San Diego played an important role in this patient-focused progress.
SOURCE: https://pmc.ncbi.nlm.nih.gov/articles/PMC5760337/?utm_source=chatgpt.com
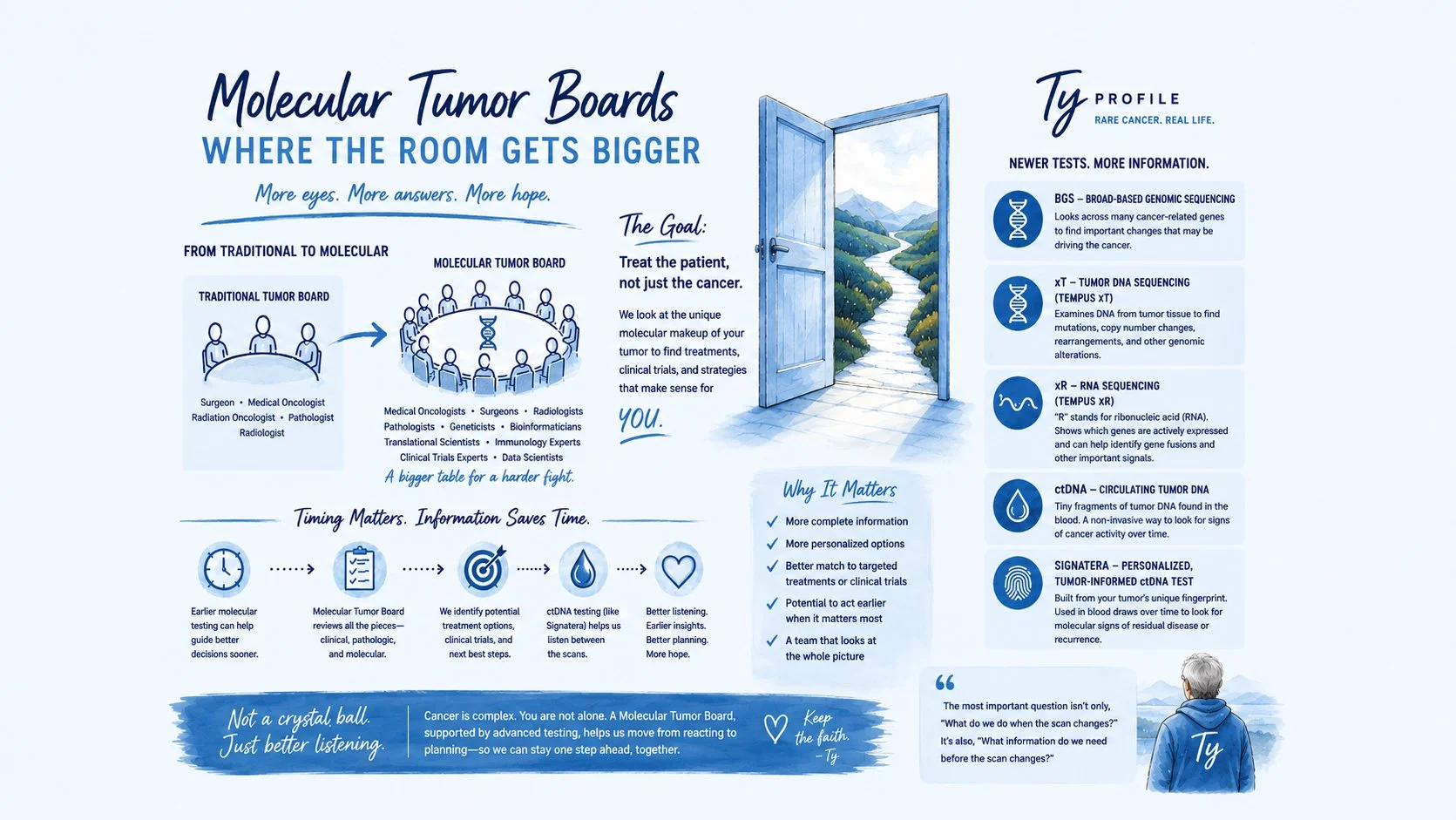
For a long time, cancer care has felt like a series of rooms. The scan room. The infusion room. The pathology room. The waiting room, which is somehow always the largest room of all. A traditional tumor board was one of the better rooms: doctors from different specialties gathered around a patient’s case and asked, “What are we seeing, and what should we do next?” But this article describes the next room opening — the Molecular Tumor Board. Same patient. Same fear. Same urgency. But now the room includes genomics, immunology, bioinformatics, pathology, radiology, clinical trials, and people who understand that cancer is not just where it appears on a scan, but what may be driving it underneath the hood.
That history matters. Tumor boards have long been one of medicine’s better ideas: put more than one set of expert eyes on a hard case. Surgeons see one kind of truth. Medical oncologists see another. Radiation oncologists, pathologists, and radiologists each bring their own lantern into the room. The Molecular Tumor Board does not replace that. It expands it. In the UCSD model described in the article, the table grew to include geneticists, bioinformatics specialists, translational scientists, immunology experts, and even supercomputer modeling. That is not just fancy medicine. That is a search party.
This matters to me because rare cancer has a way of making standard pathways feel too narrow. A Molecular Tumor Board does not promise a miracle, and I do not trust anything in cancer that comes wrapped like a miracle. What it offers is something more useful: more eyes, more disciplines, more questions, and a better chance that no important clue gets left on the floor. It asks whether a tumor’s molecular profile might point toward a targeted drug, an immunotherapy, a clinical trial, radiation, chemotherapy, or some thoughtful combination. In patient language, it asks: are we treating only the location of the cancer, or are we also paying attention to the machinery that may be helping it survive?
This is also where newer assays begin to matter. Broad-based genomic sequencing, or BGS, looks across many cancer-related genes rather than checking only one or two familiar targets. Tempus xT is a tumor DNA sequencing assay that can help identify mutations, copy number changes, rearrangements, and other genomic alterations in tumor tissue. Tempus xR means RNA sequencing, with “RNA” standing for ribonucleic acid; it can help show which genes are being actively expressed and may help identify gene fusions or other signals that DNA testing alone might miss. Circulating tumor DNA, or ctDNA, refers to tiny fragments of tumor-derived DNA that can be found in the bloodstream. In my language: broad-based genomic sequencing surveys the battlefield, xT studies the enemy’s wiring, xR listens for which wires are humming, and ctDNA looks for footprints in the hallway.
Signatera fits into this conversation in a different but important way. Signatera is a personalized, tumor-informed circulating tumor DNA test, meaning it is built from the molecular fingerprint of a person’s own tumor and then used through blood draws to look for molecular signs of residual disease or recurrence. It is not the same as a scan, and it is not a crystal ball. But for patients living between scans, ctDNA can become part of the listening system. A CT scan may show what has grown large enough to be seen. A tumor-informed ctDNA test may sometimes suggest that cancer activity is present before imaging has something obvious to point at. That does not automatically mean treatment should begin, but it may mean the conversation should sharpen.
The article’s most important warning is timing. Precision oncology is less helpful if the information arrives after the patient has already deteriorated, after the cancer has already moved, after everyone is suddenly running instead of planning. That line hit me hard. For a cancer patient, especially a rare-cancer patient, the question should not only be, “What do we do when the scan changes?” It should also be, “What information do we need before the scan changes?” A Molecular Tumor Board, supported by tools like broad-based genomic sequencing, Tempus xT, Tempus xR, Signatera, and circulating tumor DNA monitoring, can help move the conversation from passive surveillance to active planning. Not reckless treatment. Not panic. Not pretending blood tests are prophecy. Just better listening. Earlier listening.
The kind of listening that says: let’s not wait until the fire is in the hallway before we look for smoke.
—Ty
Learn to Wait…Wait to Learn
I didn't hear anything today, so I am learning about the history of ADCs. Antibody-Drug Conjugates (ADCs) are a central part of the Clinical Trial I hope to join.
My application for the ADC MATCH Clinical Trial is still being reviewed by the Principal Investigator.
So... more waiting.
Cancer teaches you that waiting is rarely passive. Waiting for scans. Waiting for pathology. Waiting for blood work. Waiting for phone calls. Waiting for treatment decisions. Waiting becomes part of the disease.
I've decided that if I'm going to wait, I might as well learn.
Today I went back to the beginning.
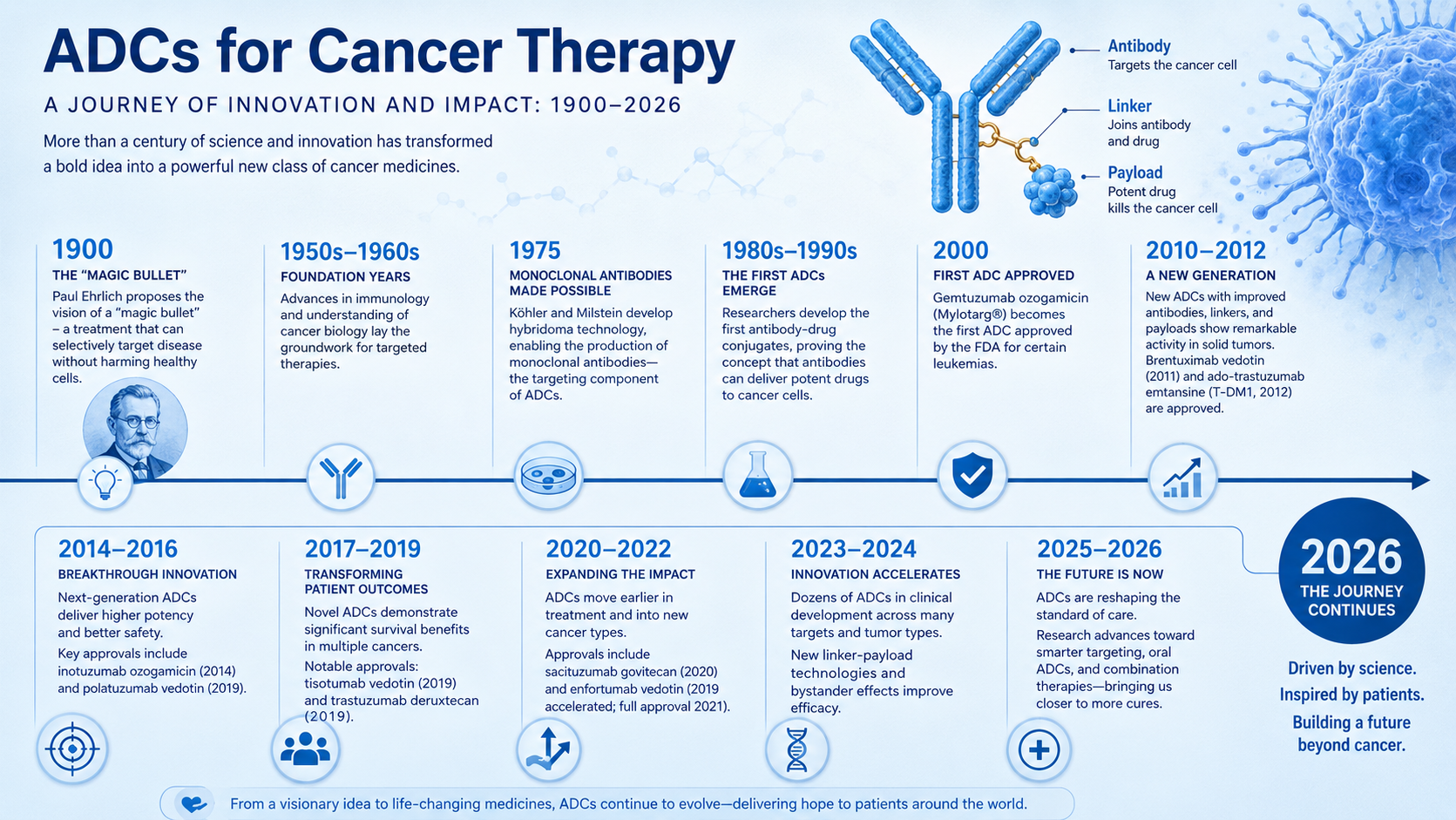
I started reading about the history of Antibody-Drug Conjugates (ADCs), beginning with the original idea of a "magic bullet" proposed by Paul Ehrlich around 1900. His vision was remarkably simple: imagine a medicine that could find only the diseased cell, leave healthy cells alone, and destroy its target with precision.
More than a century later, that vision is finally becoming reality.
I've been watching recorded lectures from oncologists and researchers discussing ADC therapy. Several of them believe that, for some cancers, targeted antibody-drug conjugates may eventually replace portions of traditional chemotherapy.
Instead of flooding the entire body with chemotherapy—as we've done for decades—an ADC uses an antibody as a guided delivery vehicle. The antibody recognizes a specific marker on a cancer cell, attaches to it, enters the cell, and releases an extremely potent drug exactly where it's needed.
It's less like carpet bombing and more like guided delivery.
One idea that really caught my attention is that the future may involve combinations of ADCs carrying different payloads. Cancer is incredibly adaptable, and one reason treatments eventually stop working is that cancer cells develop resistance.
Imagine attacking the same cancer cell in multiple different ways at the same time.
One ADC might interfere with cell division.
Another might damage DNA.
Another might activate the immune system.
Instead of relying on a single weapon, future treatments may use several highly targeted approaches together.
What surprised me most was learning that today's ADC payloads are not the same chemotherapy drugs many of us received years ago.
The medicines I received during TIP chemotherapy in 2024 and 2025 circulated throughout my body because that was the only way to reach every possible cancer cell. And the cancer still found a hiding spot.
Modern ADC payloads work differently.
Most are extraordinarily potent cytotoxic molecules—far too toxic to safely give by themselves. In the old days, these compounds would have been unusable because they would damage healthy tissue along with cancer.
But attach only a few molecules to a carefully selected antibody, and suddenly those same compounds become powerful targeted therapies. In many cases, only a handful of payload molecules need to reach the cancer cell to kill it.
As I kept reading, I discovered that ADC payloads come in several different classes.
Microtubule inhibitors interfere with the tiny structural fibers that cells use to divide. Without functioning microtubules, cancer cells cannot complete cell division and eventually die. These payloads can be 100 to 1,000 times more potent than many traditional chemotherapy drugs, which is why targeted delivery is essential.
Topoisomerase I inhibitors are one of the hottest areas of ADC development today. Rather than attacking the cell's internal scaffolding, they interfere with DNA replication and prevent rapidly dividing cancer cells from successfully copying their genetic material.
Examples include SN-38 and deruxtecan (DXd), two payloads that are already being used successfully in modern ADC therapies.
Other ADC payload classes include:
DNA-damaging agents, which break or cross-link DNA.
RNA polymerase inhibitors, which stop cancer cells from making RNA.
Protein synthesis inhibitors, which prevent cancer cells from producing the proteins they need to survive.
Immune-stimulating payloads, designed to wake up the body's immune system directly inside the tumor.
Targeted protein degraders (PROTACs), an emerging approach that causes specific cancer-driving proteins to be destroyed instead of simply blocked.
Researchers are even exploring ADCs that could deliver gene-silencing molecules, epigenetic therapies, and other precision medicines.
The more I learn, the more I realize that ADCs are becoming something much bigger than "chemotherapy attached to an antibody."
They're becoming a precision delivery platform.
The clinical trial I'm hoping to join—the ADC MATCH study—matches patients to different ADCs based on the molecular characteristics of their tumors.
The treatments currently being studied include:
• Sacituzumab govitecan, which delivers SN-38, a topoisomerase I inhibitor. If I'm matched to this treatment, this is the payload I would receive.
• Trastuzumab deruxtecan, which delivers DXd (deruxtecan), another topoisomerase I inhibitor.
• Enfortumab vedotin, which delivers MMAE, a powerful microtubule inhibitor.
Although they're all called antibody-drug conjugates, they're carrying different payloads that kill cancer cells through entirely different biological mechanisms.
Understanding the payload helps explain why two ADCs can target different cancers, produce different side effects, and sometimes work when another ADC does not.
The exciting part is that this field is still evolving.
Researchers are already investigating new payloads, smarter linkers, dual-payload ADCs, and combinations designed to reduce resistance while improving precision.
That sounds a lot like progress.
So today there wasn't a phone call.
No decision.
No acceptance into the trial.
Just another day of waiting.
But it wasn't wasted.
Every day I understand a little more about the science that may someday help me—and hopefully many others.
Maybe that's another way of fighting cancer.
One page at a time.
—Ty